Oral Semaglutide vs. Eli Lilly’s Oral GLP-1 Drug (Orforglipron): How to Choose in 2026?

In late 2025 and early 2026, oral GLP-1 therapies moved from concept to mainstream clinical reality. A key milestone came in December 2025, when the U.S. Food and Drug Administration approved the oral version of semaglutide for chronic weight management, based on Phase III OASIS data. Almost simultaneously, Eli Lilly released head-to-head Phase III results showing that its investigational oral drug, orforglipron, outperformed oral semaglutide in glycemic control and weight reduction.
This is not a routine “new drug vs. old drug” comparison. It represents a deeper shift:
From peptide biologics to small-molecule oral drugs;
From efficacy-focused innovation to adherence-focused design;
From single-target strategies to platform competition;
For clinicians and general readers, the practical question is no longer whether oral GLP-1 works, but which type is more suitable under specific real-world conditions.
1. Two Different Technological Paths: Not Just “Two Pills”
Although both drugs are taken orally and target GLP-1 pathways, their underlying technologies differ fundamentally.
1.1 Oral Semaglutide: Peptide + Absorption Engineering
Oral semaglutide is essentially the same molecule as its injectable version. Its challenge is biological: peptides are easily degraded in the gastrointestinal tract. To solve this, Novo Nordisk developed the SNAC (sodium N-[8-(2-hydroxybenzoyl) amino] caprylate) absorption system.
Key implications:
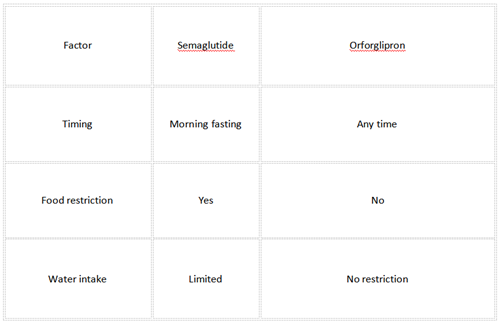
Absorption occurs in the stomach, not the intestine;
Requires fasting administration;
Must wait at least 30 minutes before eating or drinking;
Bioavailability remains relatively low despite enhancement;
This design reflects a “biological preservation” strategy—keeping the proven molecule while engineering around its limitations.
1.2 Orforglipron: Small Molecule Design
Orforglipron represents a different philosophy. It is a non-peptide, small-molecule GLP-1 receptor agonist.
Key implications:
Stable in the gastrointestinal tract;
No need for absorption enhancers;
Can be taken at any time, with or without food;
Easier to scale manufacturing (in theory);
However, synthesis is complex (reportedly ~28 chemical steps), which may influence cost and supply chain strategies.
Interpretation:
This is not just a drug comparison—it is a competition between biological mimicry and chemical innovation. The outcome may shape the next decade of metabolic drug development.

2. Head-to-Head Clinical Evidence: What the Data Actually Shows
2.1 Glycemic Control (ACHIEVE-3, 2025–2026)
The ACHIEVE-3 Phase III trial (n=1,698; 52 weeks) is the first direct comparison.
HbA1c reduction:
Orforglipron 36 mg: −2.2%
Oral semaglutide 14 mg: −1.4%
Near-normal glycemia (HbA1c <5.7%):
Orforglipron: 37.1%
Semaglutide: 12.5%
Interpretation:
Orforglipron shows stronger glucose-lowering efficacy, particularly at higher doses. The difference is clinically meaningful, not just statistically significant.
2.2 Weight Loss: Context Matters
In Type 2 Diabetes (ACHIEVE-3)
Orforglipron: up to −8.9 kg (≈9.2%)
Semaglutide: −5.0 kg (≈5.3%)
In Obesity (OASIS-4, semaglutide)
Oral semaglutide 25 mg: −16.6% body weight (64 weeks)
In obesity trials (orforglipron early data)
~12.4% weight loss (72 weeks, ATTAN-1)
Interpretation:
In diabetes populations → orforglipron appears superior
In obesity-only populations → semaglutide currently shows higher peak weight loss
This suggests that trial population and dosing strategy significantly influence perceived efficacy. It is not accurate to declare one drug universally “stronger.”
2.3 Cardiometabolic Effects
Orforglipron demonstrated improvements in:
Non-HDL cholesterol;
Systolic blood pressure;
Triglycerides;
Oral semaglutide, however, has more mature outcome data, including:
Cardiovascular risk reduction approval;
Evidence of slowing eGFR decline (SOUL trial, 2026);
Interpretation:
Orforglipron: broader metabolic signal, early-stage
Semaglutide: validated long-term outcomes
This difference reflects pipeline maturity rather than mechanism superiority.
3. Safety and Tolerability: Similar Class, Different Experience
3.1 Gastrointestinal Effects
Both drugs share class-related effects:
Nausea
Vomiting
Diarrhea
Appetite reduction
Semaglutide:
GI symptoms reported in up to ~80% of patients (mostly mild)
Orforglipron:
Similar types of side effects
Possibly stronger intensity at higher doses
3.2 Discontinuation Rates (ACHIEVE-3)
Orforglipron: 8.7%–9.7%
Semaglutide: 4.5%–4.9%
Interpretation:
Higher discontinuation may reflect:
Greater pharmacologic potency;
Faster dose escalation;
Real-world adherence challenges;
This is clinically relevant: efficacy only matters if patients continue treatment.
3.3 Long-Term Uncertainty
Both drugs still face:
Limited >5-year safety data
Ongoing cardiovascular outcome trials (for orforglipron)
FDA class warnings (e.g., thyroid C-cell tumors in animals)
4. The Often Overlooked Factor: Adherence and Real-World Use
A major insight from recent research is that drug design affects behavior as much as biology.
4.1 Dosing Burden
4.2 Clinical Implication
Studies suggest oral therapy adherence may be >3 times higher than injections in long-term use.
Within oral therapies:
Complex routines reduce adherence;
Flexibility improves persistence;
Interpretation:
Orforglipron’s main innovation may not be efficacy—but removal of friction in daily use.
5. Strategic Competition: Why This Matters Beyond Medicine
5.1 Novo Nordisk: “Deep Optimization” Strategy
Expanding semaglutide indications
Developing higher doses and combinations
Leveraging strong clinical evidence
Challenge:
Patent expiration (around 2026)
Pipeline setbacks (e.g., CagriSema expectations)
5.2 Eli Lilly: “Platform Expansion” Strategy
Dual-target drugs (e.g., tirzepatide)
Small-molecule oral drugs
Triple-target pipeline (retatrutide)
Advantage:
Diversified mechanism portfolio;
Flexible patient segmentation;
5.3 Market Projection
Oral GLP-1 may reach ~24% market share by 2030
Estimated value: ~$22 billion
Obesity treatment penetration may rise from ~3% to >15%
Interpretation:
The competition is not about replacing injections—but expanding the total treated population.

6. A Practical Selection Framework (2026)
Rather than a binary choice, selection should be context-dependent.
6.1 When Oral Semaglutide May Be Preferred
Established cardiovascular disease
Chronic kidney disease
Need for proven long-term outcomes
Higher tolerance for structured dosing routines
Preference for established clinical track record
6.2 When Orforglipron May Be Considered (Pending Approval)
Need for stronger HbA1c reduction
Desire for greater weight loss (in diabetes context)
Irregular lifestyle or difficulty fasting
Preference for simpler medication routines
Interest in newer pharmacological approaches
6.3 Situations Requiring Careful Individualization
History of severe gastrointestinal intolerance
Long-term adherence concerns
Cost sensitivity and insurance coverage
Multi-drug regimens
7. Forward-Looking Perspective: What Will Matter Next?
7.1 Beyond GLP-1 Alone
Future competition is shifting toward:
Multi-target drugs (GLP-1 + GIP + glucagon)
Combination therapies
Disease-modifying effects (e.g., cardiovascular, renal, neurological)
7.2 Expanding Indications
Ongoing research includes:
Obstructive sleep apnea
Alzheimer’s disease
Depression and metabolic-psychiatric links
7.3 The Real Definition of “Best Drug”
The emerging standard is not:
“Which drug lowers HbA1c the most?”
But rather:
“Which drug patients can take consistently, safely, and long enough to change outcomes?”
Conclusion
The comparison between oral semaglutide and orforglipron reflects a broader transition in medicine. One represents optimization of a proven biological pathway; the other represents a rethinking of drug design itself.
Current evidence suggests:
Orforglipron offers stronger short-term metabolic efficacy and greater convenience
Oral semaglutide provides more robust long-term outcome evidence and regulatory maturity
In 2026, the decision is less about superiority and more about fit—matching drug characteristics with patient needs, behaviors, and risk profiles.
The larger impact may extend beyond these two drugs. Oral GLP-1 therapies are likely to expand access, improve adherence, and redefine chronic disease management at a population level.
References:
[1] American Diabetes Association. (2026). Standards of Care in Diabetes—2026. https://doi.org/10.2337/dc26-S001
[2] Davies, M. et al. (2024). Oral semaglutide and cardiovascular outcomes in type 2 diabetes (SOUL trial updates 2026). The Lancet. https://www.thelancet.com
[3] Eli Lilly and Company. (2025). ACHIEVE-3 Phase 3 Trial Results for Orforglipron. https://www.lilly.com
[4] Novo Nordisk. (2025). OASIS-4 Trial: Oral Semaglutide in Obesity. https://www.novonordisk.com
[5] U.S. Food and Drug Administration. (2025–2026). Regulatory Updates on GLP-1 Receptor Agonists. https://www.fda.gov
Author Information
Dr. Michael Grant, MD, PhD, is a physician-scientist specializing in endocrinology and metabolic diseases. He has over 12 years of clinical and research experience in diabetes, obesity, and cardiovascular risk management. His work focuses on translating clinical trial evidence into practical treatment strategies for general populations. Dr. Grant has contributed to peer-reviewed journals and international conferences, with particular interest in GLP-1 receptor agonists and emerging metabolic therapies. He is committed to delivering accurate, evidence-based medical information in accessible language for public education.
Disclaimer
This article is intended for general educational purposes and does not replace professional medical advice. Treatment decisions should be made in consultation with qualified healthcare professionals, based on individual medical history and current clinical guidelines.
Recommended for you: